Key Points
- The majority of respondents routinely use sedation or anesthesia prior to euthanasia, with strong consensus that it is necessary for a humane outcome because it can minimize distress and adverse effects, such as wing flapping and vocalizations.
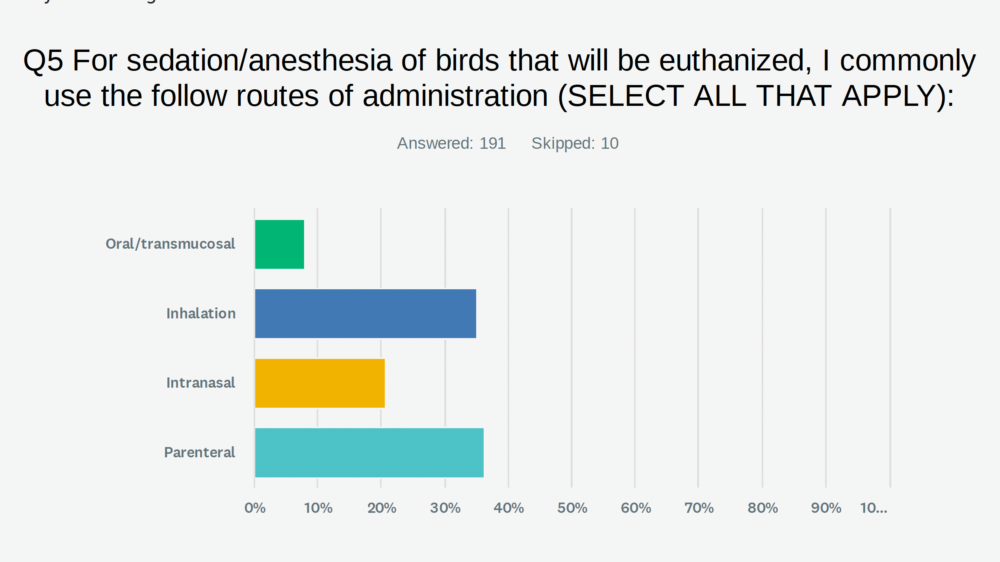
- Common sedation routes utilized by participants include intramuscular and inhalational methods, with flexible use of intranasal and oral transmucosal approaches in select cases.
- Drug protocols reported vary widely, with frequent use of combinations such as benzodiazepines, dissociatives, alpha-2 agonists, and tiletamine-zolazepam.
- Owner presence significantly influences euthanasia protocols, with many clinicians prioritizing low-stress, staged approaches and allowing client involvement when desired.
- Barbiturates (particularly pentobarbital) are the most commonly used euthanasia agents, though concerns exist regarding tissue irritation with some routes of administration.
- Intravenous administration is the preferred route for euthanasia agents, with alternatives like intracardiac injection used when necessary and typically with prior sedation.
- Many respondents provided feedback on cervical dislocation. This physical technique is used selectively, with strong emphasis on training, appropriateness, and animal welfare considerations.
Introduction
Euthanasia, or providing “a good death,” is an essential, yet often challenging, part of veterinary practice. Euthanasia presents unique difficulties in avian patients, and while many recommendations exist, strong personal opinions also shape clinical practice.
An avian euthanasia survey was shared with the LafeberVet mailing list and with LafeberVet webinar attendees during winter 2025. The survey was closed when 201 responses were received. Many respondents generously provided detailed and thoughtful feedback. View the results of this confidential survey below.
View the LafeberVet review article Avian Euthanasia: Welfare Considerations & Clinical Techniques” for additional information.
Geographic region
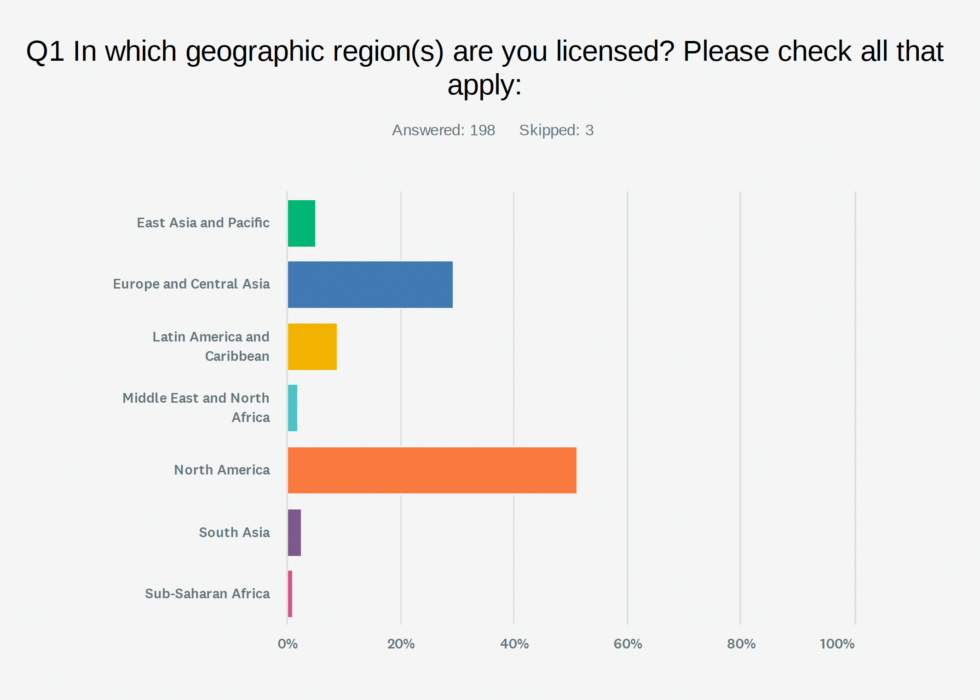
The world regions listed are based on groups defined by Our World in Data. A little over half of respondents (51.24%) are from North America. The second largest group of participants (29.35%) are from Europe and Central Asia.
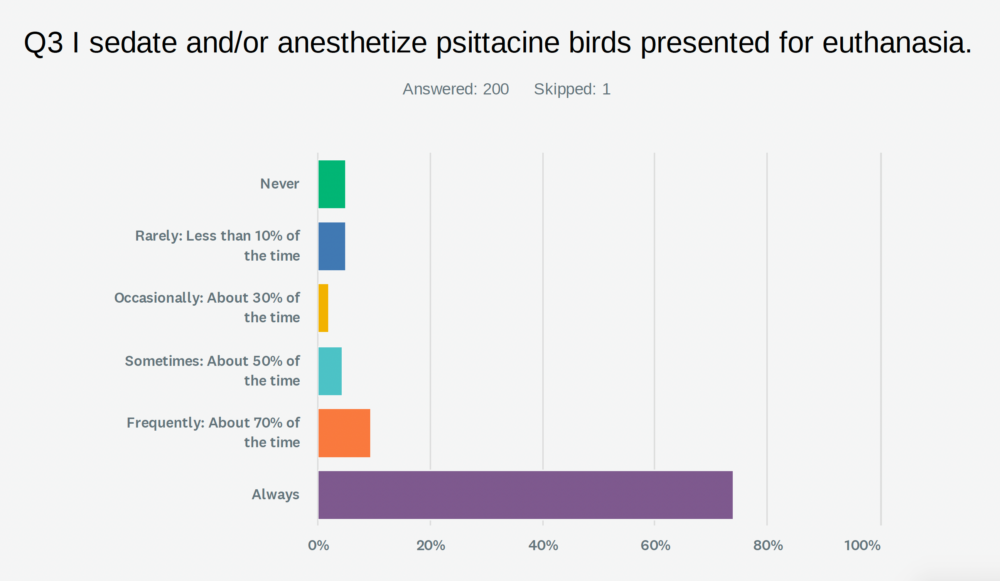
Sedation/anesthesia
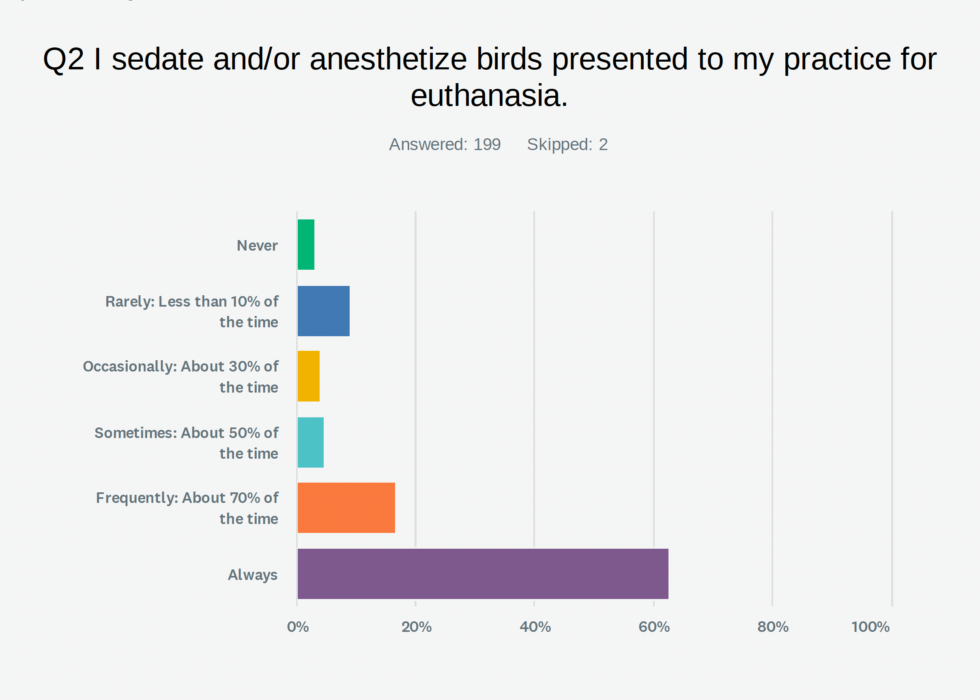
Many respondents sedate and/or anesthetize birds that present for euthanasia. Sedation and anesthesia are widely regarded as essential components of humane avian euthanasia, with the majority of clinicians reporting routine use prior to administration of euthanasia agents. Many emphasize that “deep sedation or anesthesia [is] always” performed, and that “heavy sedation or anaesthesia is an essential step prior to euthanasia”.
In fact, some practitioners note, “I always ensure my patients are under general anesthesia before administering the euthanasia agents”, underscoring the strong professional consensus around this practice. Sedation is also valued for minimizing undesirable effects associated with barbiturates, including “flapping [and] vocalization”, thereby improving both patient welfare and the client experience. Reflecting this perspective, one clinician states, “pain management and adequate sedation should be mandatory before each euthanasia”.
Sedation and anesthetic protocols are most commonly administered via parenteral or inhalational routes, with intramuscular injection frequently used for initial restraint and induction, particularly in wild or fractious birds. Inhalational agents such as isoflurane are often used to deepen anesthesia following initial sedation. Additional approaches include intranasal and, less commonly, oral/transmucosal administration (e.g., intranasal midazolam), offering flexibility in minimizing handling stress.
A variety of drug combinations are described, tailored to species and clinical context. Common protocols reported include combinations of benzodiazepines and dissociatives (e.g., midazolam/ketamine), alpha-2 adrenergic agonists with adjunct agents, and tiletamine-zolazepam–based regimens. In wildlife and field settings, injectable anesthetics such as tiletamine/zolazepam are frequently favored. Some clinicians report that high-dose anesthetic protocols, such as an overdose of propofol, may result in death without the need for a secondary euthanasia agent in severely compromised patients.
I give a whopping cocktail dose, usually of midazolam/telazol/xylazine intramuscularly (which often will result in death on its own in very ill birds-this goes over very well with owners, as it helps confirm that they have made the right decision).
I work exclusively with New Zealand wildlife…We use zoletil [tiletamine/zolazepam] for sedation. Injected IM. We make it up, draw up 0.2ml in each syringe and freeze it. Defrost as needed. Works perfectly for sedation and it is sometimes enough to euthanise…
Client presence is an important consideration influencing anesthetic approach. Many clinicians prioritize a calm, low-stress experience by allowing owners to remain with the bird during initial sedation, noting that “they are significantly sedated…then [the bird is] taken…[for] inhalational isoflurane if not completely asleep”. This staged approach balances patient welfare, client expectations, and procedural practicality.
I do not think inhalant gas should be used for anesthesia in the presence of clients, but I think birds can often be sedated parenterally or intranasally and given oral transmucosal pentobarbital if IV access is not feasible.
Almost 100% of avian euthanasias I perform are given Telazol [tiletamine/zolazepam] IM in a pectoral muscle, allowed to sit with their owner for 5-10 minutes, then given IV euthasol when deeply sedated. Works quickly smoothly and has been used by myself hundreds of times.
The vast majority of my euthanasias are performed with owner present. Most owners hold the birds following sedation and most prefer to hold them during euthanasia.
I never euthanase in front of the owner, if they want to be there while the animal goes asleep I will use intranasal midazolam and take the animal away for the injection itself.
While a minority of clinicians report performing intravenous euthanasia without prior sedation in calm patients, the prevailing standard strongly supports the use of adequate sedation or general anesthesia to ensure a smooth, humane, and low-stress euthanasia process across avian species.
In clinical practice I predominantly use intravenous euthanasia via the medial metatarsal vein, which is reliable in most species and often does not require sedation when performed calmly and efficiently. Sometimes, due to diagnostic work such as radiography, I will sedate first using an intramuscular protocol of medetomidine, butorphanol, and alfaxalone.
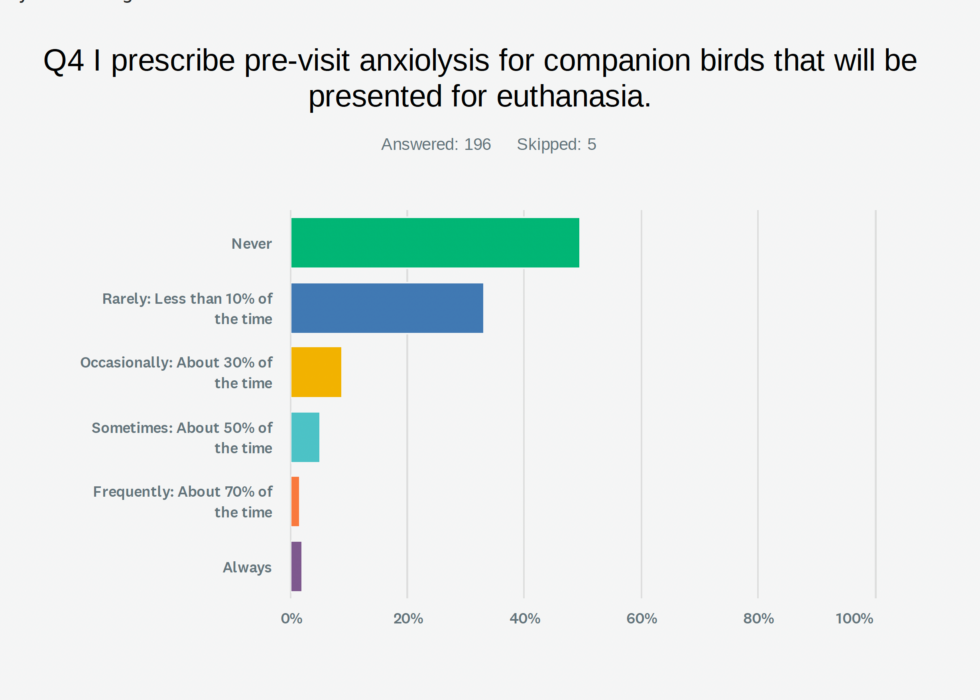
Most respondents do not use pre-visit anxiolysis. As one respondent shared, “Pre-visit anxiolysis is rarely practical”.
Routes of administration
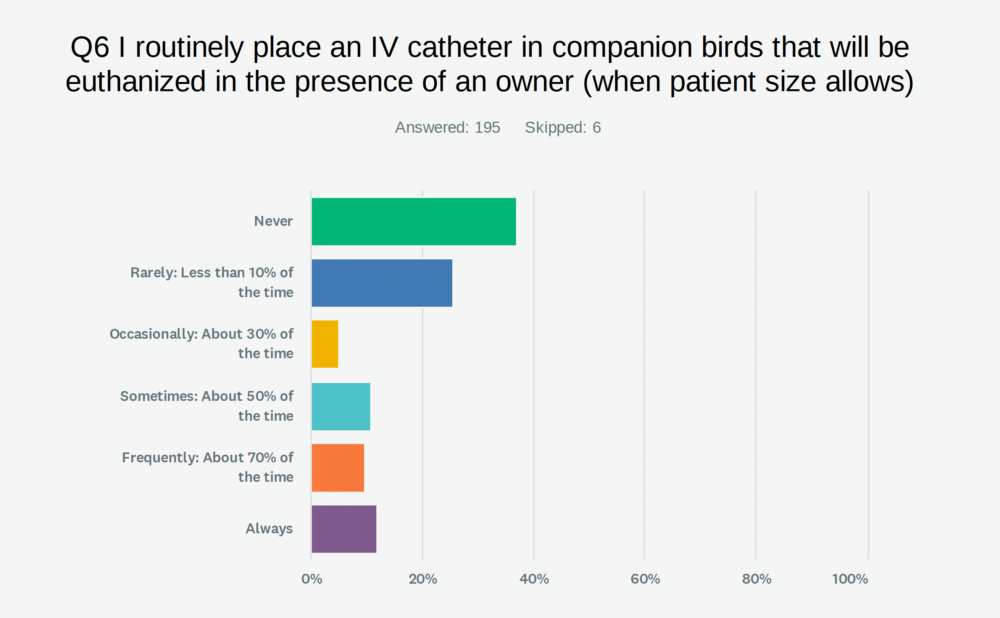
For birds euthanized in the presence of an owner, a majority of respondents (36.92%) never place an IV catheter
I think it is important that clinicians make every effort to allow clients to be present for euthanasia if that is desired.
I do not think inhalant gas should be used for anesthesia in the presence of clients, but I think birds can often be sedated parenterally or intranasally and given oral transmucosal pentobarbital if IV access is not feasible.
I think it is important that we never say clients cannot be present if that is what they desire.
The vast majority of my euthanasias are performed with owner present. Most owners hold the birds following sedation and most prefer to hold them during euthanasia.
I never euthanase in front of the owner, if they want to be there while the animal goes asleep I will use intranasal midazolam and take the animal away for the injection itself.
Euthanasia agents
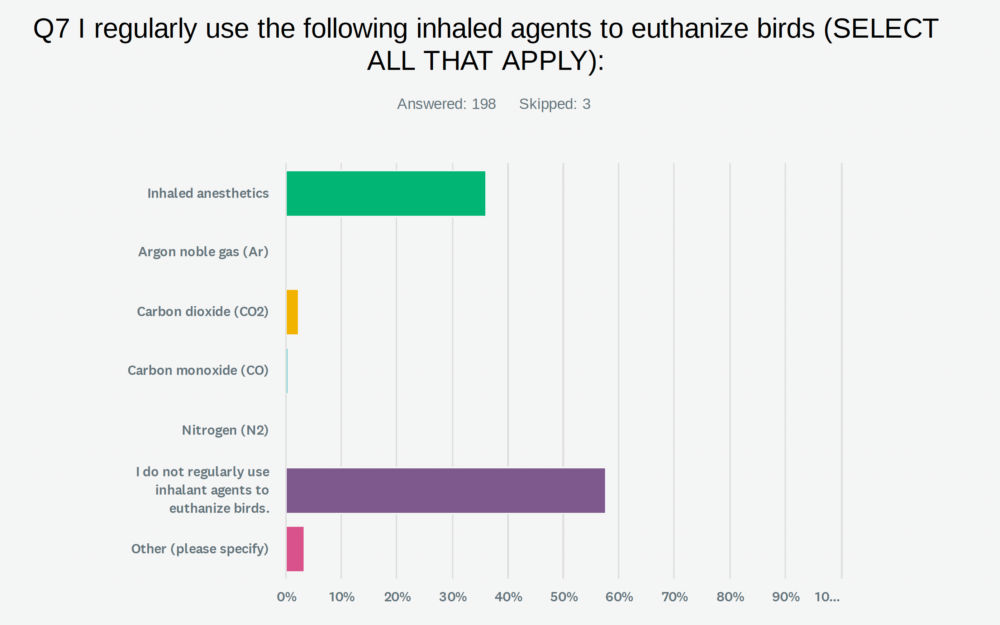
Euthanasia agents are usually administered via parenteral routes (36.34%) or inhalation (35.05%). When using inhaled agents, survey participants report that birds may become unconscious very quickly, with one respondent noting they are “asleep within three breaths”. Delivery of isoflurane via induction chambers or enclosed environments is designed to avoid direct contact with the liquid anesthetic and is associated with “less struggling than anesthesia by mask”.
I euthanize [by] pouring isoflurane into a Rubbermaid® box in a vent hood…
For small birds…We use Ziploc® bags, place the anesthetized bird in the bag with a small piece of gauze and then inject isoflurane onto the gauze. We then cover with a towel and allow about 10-15 minutes before we confirm death. This method is especially useful if there is only one person licensed to handle euthanasia drugs in our wildlife clinic.
Therefore, inhalant techniques also offer logistical advantages in wildlife and field settings, particularly when access to controlled euthanasia agents is limited or restricted. Such methods also reduce the need for physical restraint, thereby minimizing stress in free-ranging or fractious birds.
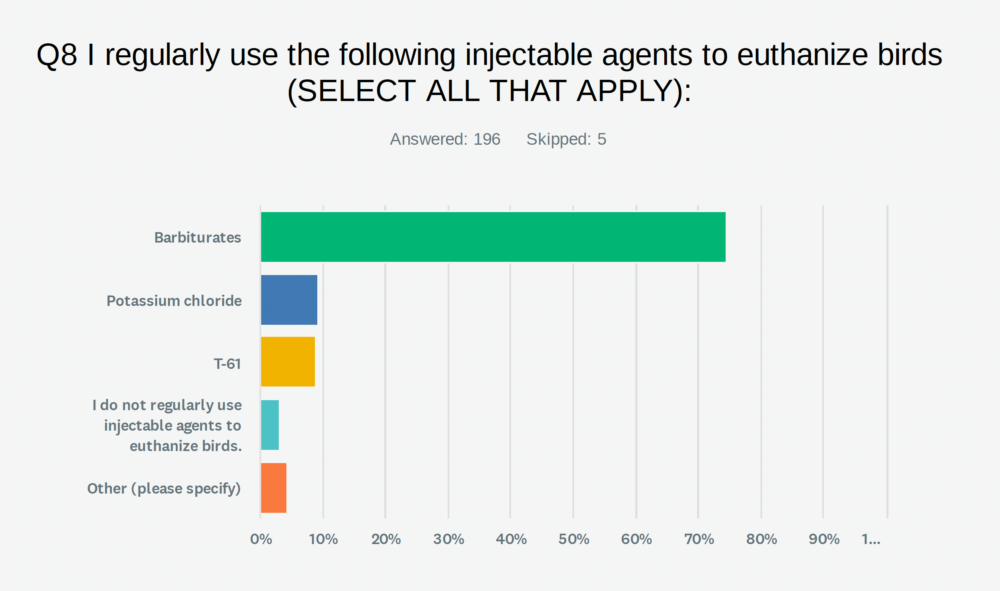
Barbiturates are used most commonly (74.45%). A few respondents recommend diluting pentobarbital half strength.
[I] find that full strength causes more vocalisation, muscle spasms, agonal gasping etc.
There were also conflicting opinions expressed on T-61:
It would be helpful to bring T-61 back to the USA. With pre-sedation this is a humane drug.
…I know there are studies stating that T-61 is humane for euthanasia because this drug contains a paralytic, I personally do not think it should ever be used. No matter what studies say, if there is a chance, however slight, that an animal is paralyzed before it undergoes cardiorespiratory arrest, we should not use that method. Is this something you would risk on your pet? I certainly would not.
One respondent shared their preferred regimen with potassium chloride.
Usually, I use propofol and potassium chloride after the animal is tranquilized and with pain killers.
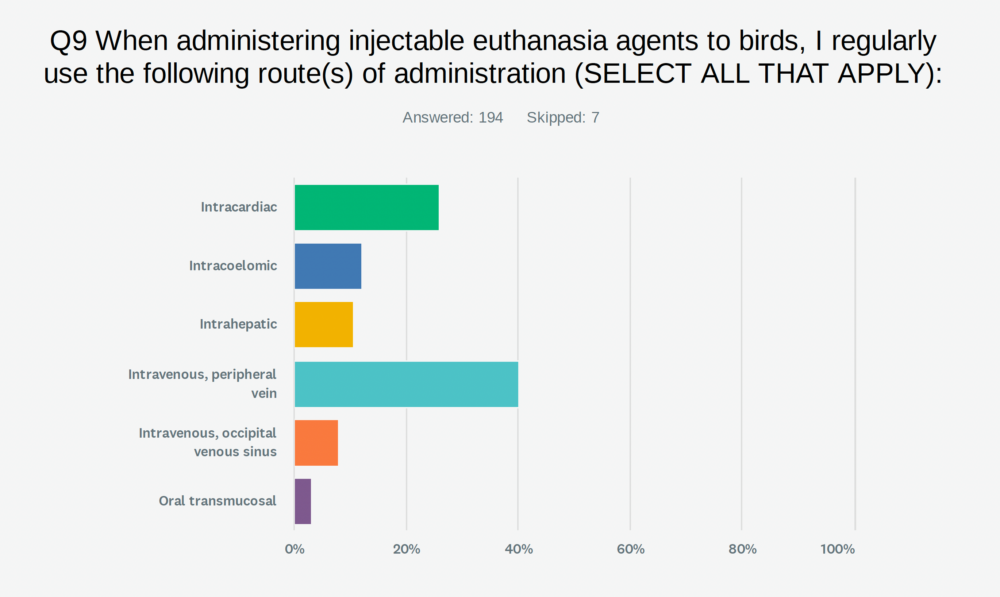
There is strong consensus that the intravenous (IV) route via a peripheral vein is the preferred and most commonly utilized method. Clinicians frequently report administering agents through accessible sites such as the ulnar or medial metatarsal veins, noting that this approach is “reliable in most species” and can be performed efficiently, sometimes without sedation in calm patients. In wildlife and clinical settings alike, peripheral IV catheterization is widely used.
The intracardiac route is the second most reported method in some contexts, though used less frequently overall. Its application is generally limited to anesthetized or deeply sedated patients:
Sedation is key prior to intracardiac administration, especially in a setting with the owners. Be as fear free as possible to make the birds last moments stress less.
Another clinician stressed the importance of intracardiac injections in veterinary training, particularly for wildlife applications:
I urge all veterinarians and attempt to teach veterinary students intracardiac injections on wild birds for euthanasia so they feel more comfortable providing that service to animals in whatever practice they choose.
Greater variability in administration routes is observed in small or pediatric birds. Oral administration of barbiturates may be appropriate in select cases, particularly when birds are still voluntarily eating, with one clinician noting it as “lowest stress…[and] excellent for owner experience.” Delivery via crop needle or feeding tube is also described as “effective and fast, minimizing handling for wild birds”.
The occipital venous sinus has been used to achieve rapid unconsciousness.
I don’t know how often I actually hit the occiputal venous sinus but what I suspect is happening – either flooding the brain with pentobarb and/or hydrostatic pithing – appears to cause reliable unconsciousness in under a second and – as the target area is larger – requires only very brief restraint. There is frequently wing spasm so not recommended for birds whose owners are present.
Additional routes—including intramuscular, cloacal (intracloacal), subcutaneous, and intrathecal administration—are reported with mixed perspectives. Some clinicians describe intramuscular administration as “consistent, pain free, [with] smooth ‘induction’ and death within 5 minutes”, while cloacal administration is considered by others to be “very effective…[with] little stress or pain,” particularly in small birds and poultry. Subcutaneous administration has also been noted to allow birds to “fall asleep…without showing any distress” in certain companion species. Intrathecal administration of lidocaine, performed under anesthesia, is reported to produce “quick death and no signs of pain”.
Unfortunately, the option for intramuscular euthanasia is not given [in the survey], and this is my preferred route of administration, which works very well [using] T61 (31 years of experience with this route).
Cloacal pentobarb [is] useful in companion birds (psittacines and pet chickens).
I mainly deal with wild birds. Giving pentobarb per rectum seems very effective, and seems not to cause much stress or pain. (Doesn’t work well in aquatic birds, I always use IV for these patients).
I have used pentobarbital injected SQ in small birds such as budgies and cockatiels and it has worked very well. Owners can stay with the bird and they just fall asleep and then die without showing any distress.
Despite these varied practices, important welfare considerations are highlighted.
Pentobarbital is extremely irritating to mucosa and therefore oral, cloacal, intracoelomic and intramuscular routes are inappropriate and do not meet the criteria for euthanasia “a good death”. If methods other than intravenous administration are used, patients must be anaesthetised.
Q10-Q13. My preferred route for administration of injectable euthanasia agents given to…
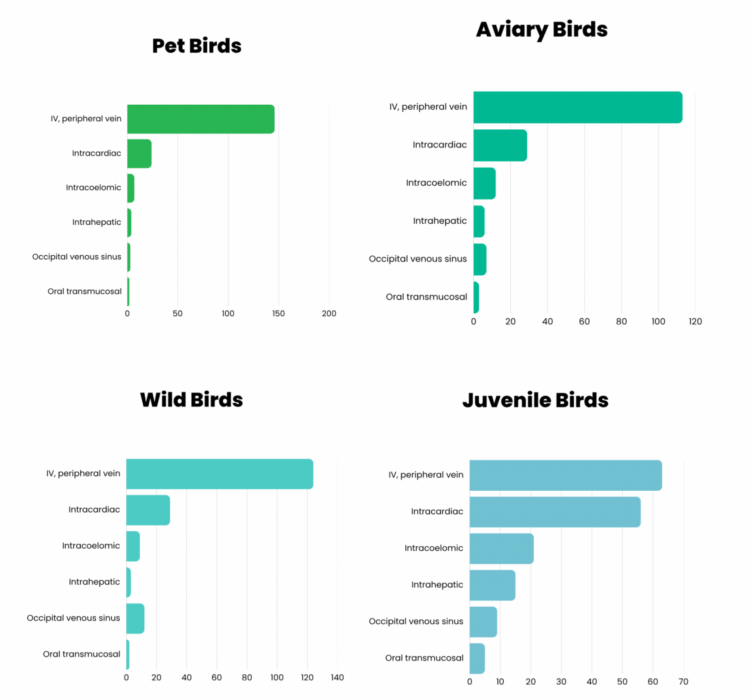
The preferred route of administration is quite similar across companion, wild, and aviary birds, with use of a peripheral vein being most popular and intracardiac being secondary. A bit more variety is incorporated into the approach to euthanasia of juvenile birds. (See the PDF below for details).
Download the detailed survey results
Download the PDF version of survey results for questions 1-13 listed above, including details on the preferred route of administration for companion birds, wild birds, juvenile birds, and aviary birds.

Clinical tips
Q14. Are there any clinical tips or comments on avian euthanasia that you wish to share?
Several respondents shared comments about poultry:
Chickens are still a challenge due to their tendency to stretch their legs and flap immediately following death, which is disturbing to owners (we warn them if they elect to be present), we are still working on dosing to avoid this.
…I think it is important to give chickens sufficient sedation and/or propofol prior to euthanasia to prevent vocalization/dysphoria.
Important to note that [a] recent study showed that oral transmucosal pentobarbital is poorly effective for euthanasia in chickens; this is in line with my personal experience in chickens.
…Or perhaps you regularly use physical methods, such as cervical dislocation?
The comments received confirm that cervical dislocation is used as a euthanasia method in avian species under specific conditions. Most commonly, it is performed in field settings where access to anesthetic or euthanasia agents is unavailable, or when rapid intervention is required. A few respondents in wildlife or rehabilitation settings select this technique when carcasses may be repurposed as food for other animals. This practice was also reported in research or academic settings.
Additional applications reported included situations where preservation of tissue for pathology is necessary and management of suspected infectious diseases to limit in-clinic exposure. In backyard poultry operations, one participant also shared that cervical dislocation may be selected to reduce stress-related biochemical changes in meat.
We are a wildlife hospital…if [the] patient has no disease or medication, [cervical dislocation] can be used as natural food for other patients (birds of prey, foxes, etc).
[I] have used cervical dislocation in wild birds with suspected infectious diseases that we don’t want inside the practice.
I use dislocation on backyard poultry farms (chickens, ducks, turkeys, and quail) because it greatly reduces cortisol contamination in the meat.
Cervical dislocation is primarily reserved for appropriately-sized birds, including neonates or small wild birds. This technique is also used in poultry, such as chickens, turkeys, and quail.
We regularly use cervical dislocation for birds corvid and smaller. Mostly pigeons or small garden birds.
I’ve used cervical dislocation in newly hatched chicks and ducklings (in a teaching/academic/research setting), and while emotionally disturbing, I believe it works well.
Cervical dislocation is generally avoided in larger species, such as waterfowl and raptors, although a few respondents specifically mentioned the application of this technique in these relatively large birds.
…in chicken…cervical dislocation is my choice.
[I] wouldn’t use cervical dislocation in waterfowl, raptors etc.
Proper training of veterinary professionals, wildlife staff, and, in some cases, experienced animal handlers was emphasized by some respondents.
Once trained on this method it is fast and in my opinion, humane for smaller birds…
…Any bird bigger than [a] wood pigeon I will always gas down with iso[flurane] beforehand.
[I perform] cervical dislocation in smaller birds after inhalation anaesthesia.
Whilst this may be controversial, I am confident in mechanical euthanasia techniques as they are useful in the field where it is not practical to carry anaesthesia/euthanasia products. I also encourage my colleagues and certain clients (e.g. falconry clients) to learn it in case they have an emergency requiring immediate euthanasia of one of their birds and they are a distance from a veterinary centre.
As a wildlife vet, I also need to ensure my team are competent in physical methods of euthanasia. Therefore, I do teach cervical dislocation for appropriate small species, but only with proper training and assessment
Of course, not everyone recommended this technique:
I have never used physical methods, and I do not think they should be used unless there is no other option. With chemical euthanasia, each step of the process reduces pain/distress, while with physical methods, if the method is performed incorrectly, it can result in severe pain and distress.
Pollock CG. Avian euthanasia survey results. LafeberVet website. April 8, 2026. Available at https://lafeber.com/vet/avian-euthanasia-survey-results/