Video
Video produced by M. Scott Echols, DVM, DABVP (Avian Practice) and narrated by Marla Lichtenberger, DVM, Dipl. ACVECC. Video script adapted from Dr. Paul-Murphy’s article by Christal Pollock, DVM, DABVP (Avian Practice). Video script reviewed by Drs. M. Lichtenberger , M.S. Echols, Natalie Antinoff, DVM, DABVP (Avian Practice) and S. Orosz, DVM, DABVP (Avian Practice), DECZM.
Introduction
When a rabbit is weak, dehydrated, and has been anorectic for more than 24 hours, use of a nasogastric (NG) tube can be less stressful and more successful than syringe feeding (Fig 1). Nasogastric intubation is also indicated in rabbits that will undergo surgery involving the oral cavity, esophagus, stomach, or biliary tract. Enteral feeding is an essential component in recovery from illness, as it delivers calories, rehydrates stomach contents, promotes gastrointestinal motility, and prevents hepatic lipidosis. Overweight, anorectic rabbits are particularly at risk for developing hepatic lipidosis.

Figure 1. Nasogastric tube placement can be more successful than syringe feeding in the weak, dehydrated rabbit that has been anorectic for more than 24 hours. Click image to enlarge.
Equipment needed
- 3.5-to 8-French soft, flexible, pediatric feeding tube (Argyle tube, Kendall Company). This tubing is softer than a red rubber tube, and a stylet is not necessary. Select an 8-French tube for larger rabbits (Oryctolagus cuniculus) and a 5-French tube for large guinea pigs (Cavia porcellus). Use a 3.5-French tube in small guinea pigs.
- Local anesthetic (i.e. 2% lidocaine gel, lidocaine viscous, or proparacaine hydrochloride)*
- Syringe, 6-12 mL
- Water-based lubricant
- Tape
- Suture material or surgical staples, white porous tape, and needle holders, or surgical glue and latex glove
Technique for nasogastric tube placement in the rabbit:
- Determine the length of tubing necessary to reach the stomach by measuring from the tip of the nose to the last rib (Fig 2). Mark this point with a piece of tape on the tube or with a permanent marker. Determine the volume needed to flush the tube.

Figure 2. Determine the tube length needed to reach the stomach by measuring from the tip of the nose to the last rib. Click image to enlarge.
- Place a local anesthetic into the rabbit’s nares at least 2-3 minutes before tube placement. Instill both nostrils in case tube placement must be attempted in the other naris. Briefly elevate the head to promote coating of the nasal mucosa with local anesthetic (Fig 3).

Figure 3. Instill a local anesthetic into both nares. Click image to enlarge.
- Have an assistant properly restrain the rabbit. Protect its back and flex the head ventrally, ensuring the neck is straight to avoid tracheal compression.
- With a generous amount of lubricant at the tip of the feeding tube, gently insert the tube ventromedially into the ventral nasal meatus(Fig 4). Do not use a stylet, as the esophageal mucosa is delicate and easily torn.

Figure 4. Tilt the head up to gently insert the tube into the ventral nasal meatus.
Direct the tube ventromedially. Click image to enlarge. - Rabbits that will not tolerate nasogastric intubation with topical anesthetic alone will need heavy sedation or light anesthesia to place the nasogastric tube.
- Advance the tube until the end reaches the stomach (previously marked in Step #2)(Fig 5).

Figure 5. Once the tube is in the ventral nasal meatus, place the neck in a normal, flexed position to allow the tube to slide into the oropharynx and esophagus instead of the trachea. Click image to enlarge.
If resistance is met, gently withdraw the tube and attempt to pass it while gently rotating the tube. If the tube still cannot pass, then place the tube in the other nostril. Occasionally an elongated tooth root can cause resistance.
- Verify tube placement using more than one method:
- Aspirate gastric contents.
- Take a survey lateral radiograph to confirm tube position (Fig 6). Some tubes have a radiodense marker or a small amount of non-iodinated contrast material can be instilled into the tube if need be.
- The tube may also be palpated within the esophagus, although this is difficult with small diameter tubes.
- Air may also be injected through the tube while the stomach is ausculted for a gurgling sound.
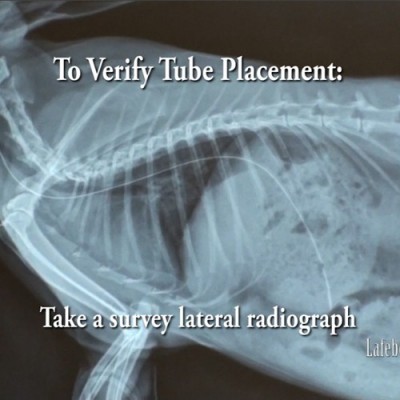
Figure 6. One method to verify tube placement is to take a survey lateral radiograph. Click image to enlarge.
*** Do not rely upon flushing the tube with water, as a depressed or sedated rabbit will likely make no coughing sounds if the tube is in the trachea.
- Secure the tube to the nose using tape tabs and suture (Fig 7), or secure it further along the length of the tube between the ears where surgical staples can be applied (Fig 8).

Figure 7. The tube can be secured to the nose using butterfly tape and suture. Click image to enlarge.

Figure 8. The nasogastric tube can also be secured between the ears. Click image to enlarge.
Another method uses surgical glue and a cut piece of latex glove. Insert your index finger into a latex glove and place the finger firmly over the tube as it passes over the rabbit’s nose. Liberally apply surgical glue between the glove and the tube, holding the tube in place until the glue has begun to set. Then carefully remove your finger from the glove, trimming all but a small patch that overlies and anchors the tube.
- Curve the tube up between the eyes and ears and along the back of the head.
- Cap the tube opening to prevent air from building up within the stomach.
- Rabbits generally tolerate NG tubes well, and it is best to avoid surgical collars for rabbits. However, if necessary, use of a soft, recovery collar will prevent premature tube removal and is usually well tolerated.







Tube feedings
Deliver Emeraid Intensive Care Herbivore or Emeraid Sustain Herbivore slowly by syringe into the NG tube every 6 hours. Use a small syringe (i.e. 3 ml or smaller) to minimize the pressure on the small-diameter tube (Fig 9). Emeraid IC Herbivore is a partially elemental diet designed for the critically ill herbivore, so it is particularly well suited for feeding a rabbit that requires NG tube placement. Emeraid Herbivore easily passes through a 5-French tube; the formula must be diluted slightly to pass through a 3.5-French tube (Marla Lichtenberger, personal communication, June 21, 2011). Critical Care Fine Grind (Oxbow Animal Health; Murdock, NE) is an alternative product.

Figure 9. Using a small syringe, slowly deliver food every 6 to 8 hours to minimize pressure on the small-diameter nasogastric tube. Click image to enlarge.
Follow every feeding with at least 5-6 ml of water to keep the tube patent, and monitor the rabbit carefully for stool production. Slightly soft droppings are typically seen within 12-36 hours.
Continue to offer greens, grass hay, and water free choice as the rabbit can still eat, drink, and swallow around the tube.
Tube removal
The NG tube may be left in place for weeks or until the rabbit is eating on its own and producing stool. The tube is easily removed in the conscious rabbit.
Contraindications and potential complications
Absolute contraindications for NG intubation include severe trauma to the midface or recent nasal surgery. Relative contraindications are also quite rare and include coagulopathy, esophageal stricture, and alkaline ingestion.
In human medicine, reported complications vary widely from 0.3% to 8.0%. The most common problems are tube-related and include tube knotting and impaction, the tube doubling back and kinking, tube breakage, or tube obstruction and rupture with syringing. Epistaxis may also occur, but generally can be avoided by generously lubricating the tube tip and using gentle technique. Nasal discharge can also be observed with tube irritation or contamination of the lower respiratory tract. In these instances, remove the tube and implement antibiotic therapy (Fig 10). Other potential albeit uncommon complications include bronchial placement leading to atelectasis, pneumonia and lung abscess. In some rabbits, tube or collar placement can also be extremely stressful for the severely debilitated rabbit leading to secondary gastrointestinal stasis.

Figure 10. Remove the tube immediately if nasal discharge develops. Click image to enlarge.
References
References
Brown C. Nasogastric tube placement in the rabbit. Lab Anim 39(1):14-15, 2010.
Paul-Murphy J. Critical care of the rabbit. Vet Clin North Am: Exot Anim Pract 10(2):437-461, 2007.
Pillai JB, Vegas A, Brister S. Thoracic complications of nasogastric tube: review of safe practice. Interact Cardio Vasc Thorac Surg 4(5):429-433, 2005.
Paul-Murphy J. Nasogastric tube placement in the rabbit. March 25, 2013. LafeberVet Web site. Available at https://lafeber.com/vet/nasogastric-tube-placement-in-the-rabbit/